A medical negligence case in India runs through three separate doors, and they do completely different things: the consumer commission awards compensation, the criminal court punishes gross negligence, and the medical council acts against the doctor's licence. Families routinely lose years by knocking on the wrong door first, usually the police station, when what they actually want is accountability and compensation. In July 2026 the Supreme Court sharpened the line again, reaffirming that a doctor cannot be criminally prosecuted for negligence without an independent expert medical opinion supporting the allegation. This guide maps all three doors: the legal tests, the forums and their monetary limits, the two-year limitation, the evidence that decides these cases, and what Indian courts actually awarded in 2026, from ₹1 lakh for a poorly treated kidney stone to ₹2 crore for a wrongly removed kidney.
Key takeaway: decide what you want before you decide where to file. Compensation lives in the consumer commissions. Punishment lives in the criminal courts, behind a deliberately high gate. Licence action lives with the medical councils. Each door has its own test, its own clock and its own evidence, and choosing the wrong one costs years.
What "medical negligence" legally means
Negligence in Indian medical law is a failure of reasonable care, judged against what an ordinarily competent practitioner in that specialty would have done. The standard descends from the English Bolam test and has been consistently applied by the Supreme Court since Jacob Mathew v. State of Punjab, (2005) 6 SCC 1. Three consequences follow, and each one kills a category of weak cases:
- A bad outcome is not negligence. Medicine has complications without carelessness. The NCDRC applied exactly this in July 2026 when it set aside orders against a dermatologist and plastic surgeon because a hair treatment merely failed to produce results.
- An error of judgment is not negligence if a competent body of professional opinion could have made the same choice between accepted alternatives.
- The duty attaches to the process, not the promise. Doctors owe care in diagnosis, treatment choice, warning of risks (informed consent), and post-operative attention; they do not insure results.
What converts tragedy into liability is a breach of that process standard which causes the harm: an operation on the wrong organ, an instrument left inside, a warning never given, a deteriorating patient left unattended. Duty, breach, causation, damage: all four must line up.
Door 1: the consumer commission (compensation)
Since Indian Medical Association v. V.P. Shantha, (1995) 6 SCC 651, paid medical treatment is a "service", and negligent treatment is a deficiency in service under the Consumer Protection Act, 2019. This is the door for compensation, and it is where the overwhelming majority of successful medical negligence cases in India are fought.
| Forum | Claim value | Where it sits |
|---|---|---|
| District Consumer Commission | Up to ₹50 lakh | Your district; file on e-Daakhil or at the registry |
| State Consumer Commission | ₹50 lakh to ₹2 crore | State capital benches |
| NCDRC (National Commission) | Above ₹2 crore | New Delhi |
Essentials of this door:
- Limitation: two years from the cause of action (the negligent act or, where injury reveals itself later, its discovery), with condonation possible on sufficient cause. Anger does not pause this clock; funerals and second opinions consume it fast.
- Fees are modest and nil for claims up to ₹5 lakh; filing is online via e-Daakhil.
- Expert evidence wins it. Filing does not strictly require a prior expert opinion, but proving breach almost always does, and commissions weigh the independence of the expert: a government medical board or an unconnected teaching institution carries far more weight than a colleague from the same hospital.
- Hospitals are on the hook too. Institutions are vicariously liable for their staff and consultants, and directly liable for systemic failures (instrument counts, infection control, absent emergency cover). "He was only a visiting consultant" is not an exit.
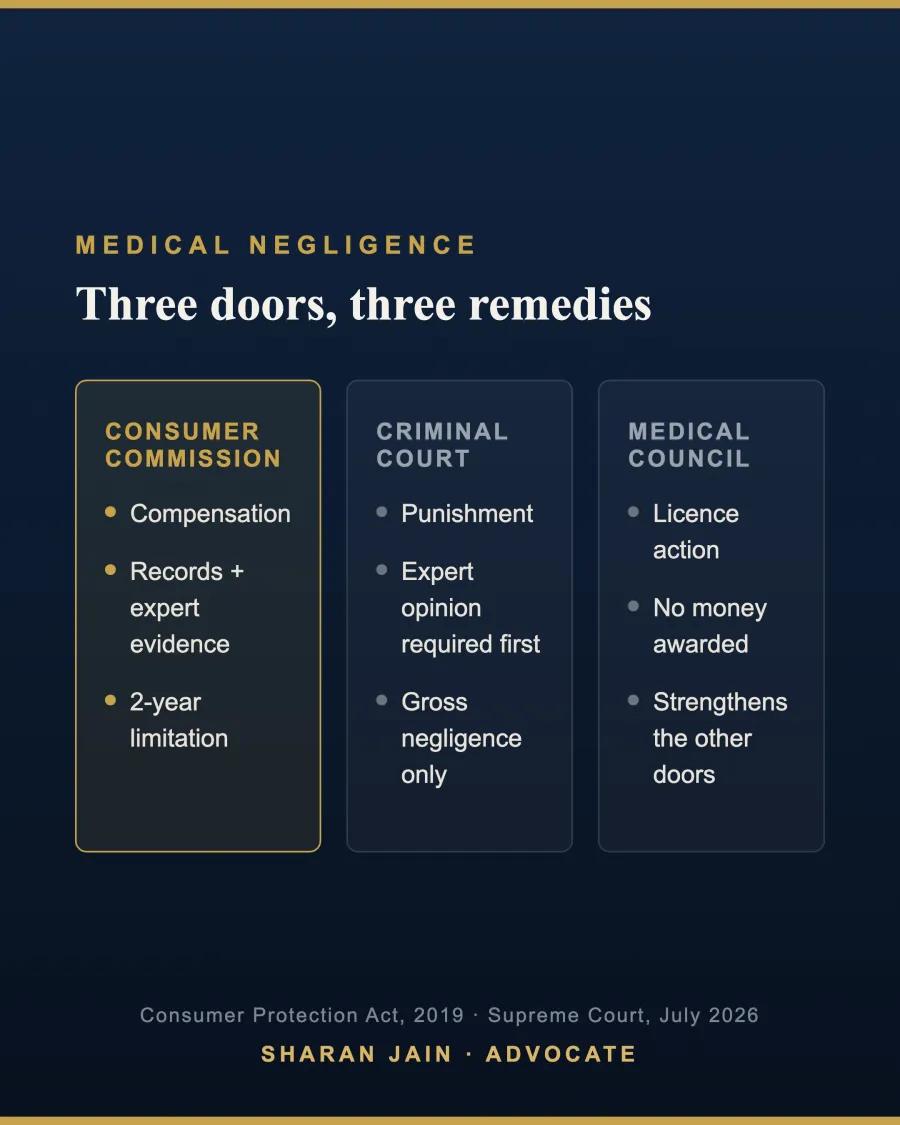
Door 2: the criminal court (punishment, behind a high gate)
Criminal liability needs gross negligence, recklessness of a degree that a court considers deserving of punishment, not a mere lapse. Jacob Mathew laid down the safeguard that has had to be repeated for twenty years: before a doctor is prosecuted, the allegation should be supported by credible, independent medical opinion, and doctors should not be arrested routinely. In July 2026 the Supreme Court reaffirmed the rule, insisting on an independent expert opinion before prosecution proceeds, precisely because FIRs against doctors continue to be registered on grief rather than evidence.
Understand what this door does and does not do. A conviction punishes the doctor (imprisonment or fine under the negligence provisions of the criminal code); it pays the family nothing. It exists for the rare case that crosses from carelessness into culpable recklessness: operating under intoxication, treating far outside competence, abandoning a critical patient. If your real goal is compensation, this door is not merely slow; it is the wrong building.
Door 3: the medical council (the licence)
The National Medical Commission and the state medical councils enforce the Registered Medical Practitioner (Professional Conduct) framework. A council complaint can end in a warning, suspension, or removal from the register, and it costs nothing to file. No compensation is possible here, but a council finding of professional misconduct powerfully corroborates a consumer case, and for dangerous practitioners it is the only door that stops the next patient from being harmed. Complaints go to the state council where the doctor is registered, with an appeal to the NMC's Ethics and Medical Registration Board.
What courts actually awarded: the 2026 spectrum
Numbers communicate the system better than doctrine. From this year alone:
- ₹2 crore for the removal of the wrong kidney (Aligarh), after a twelve-year fight; errors of this class speak for themselves, and the doctrine of res ipsa loquitur shifts the burden to the hospital.
- ₹50 lakh ordered against a doctor and hospital for negligence in a 23-day-old infant's treatment (July 2026).
- ₹12.7 lakh by a Maharashtra consumer court for a surgical mop left inside a patient (July 2026): instrument counts are a system duty, so the institution answers.
- ₹17.95 lakh recommended by the Maharashtra State Human Rights Commission for a childbirth death in a public facility, a reminder that human rights commissions are a further forum where state hospitals are involved.
- ₹1 lakh upheld by the Delhi State Commission for a poorly treated kidney stone: modest deficiency, calibrated award.
- Zero in the NCDRC's hair-treatment ruling: no result is not negligence.
The full breakdown of how these figures are computed, loss of income and dependency, treatment costs, pain and suffering, is in our companion guide to medical negligence compensation amounts in 2026.
Building the case: the evidence sequence
Whichever door you choose, the case is built in the first month, usually while the family is still in shock. The sequence that works:
- Get the complete medical records, in writing, immediately. You are legally entitled to them; the NMC's professional conduct regulations require hospitals to supply records on request within a fixed period. Ask for admission notes, operation notes, anaesthesia records, ICU charts, discharge summary and bills, and keep the acknowledgment of your request.
- Preserve everything contemporaneous: prescriptions, consent forms (what exactly was consented to, and when it was signed), diagnostic films, payment receipts, and your own dated notes of conversations.
- Obtain an independent expert opinion from an unconnected specialist or a medical board. It is now mandatory before the criminal door opens, and it is the spine of the consumer case: it must speak to both limbs, the deviation from the standard of care and the causation of the specific harm.
- In death cases, insist on a post-mortem where cause of death is unclear. It is painful and it is often decisive.
- Then choose the door, with the two-year consumer limitation in mind.
Common mistake: filing an FIR first "to pressure the hospital", then arriving at the consumer commission years later with a stale claim and no records. The criminal case will stall at the expert-opinion gate; the consumer clock will have run. Secure records and expert opinion first; choose forums second.
A practice note on what actually decides these cases
Having watched these disputes from the lawyer's chair: the medical record is usually the verdict. Courts reconstruct clinical judgment years later entirely from what was written at the time, and a sound decision poorly documented is indistinguishable from a poor decision. That cuts both ways. Families with a genuine case should not fear a paper war; the gaps, overwrites and missing consent forms in a bad record are themselves evidence. And the case that settles or wins is almost never the angriest one; it is the one with a complete file, an independent expert who addresses causation squarely, and a claim valued on documented loss rather than grief. Value the claim honestly, plead the heads of loss specifically, and start inside the limitation period with room to spare.
Frequently Asked Questions
Where should I file a medical negligence case in India?
For compensation, the consumer commission matching your claim value: district up to ₹50 lakh, state up to ₹2 crore, NCDRC above that. Criminal complaints are reserved for gross negligence and now require independent expert support. Council complaints target the doctor's registration.
What is the time limit for a medical negligence complaint?
Two years from the cause of action for consumer complaints, extendable only on sufficient cause shown. Council and criminal processes have no such fixed bar, but delay degrades evidence everywhere.
Can a doctor be arrested on a family's complaint alone?
No. Since Jacob Mathew (2005), reaffirmed by the Supreme Court in July 2026, criminal prosecution for medical negligence requires an independent expert medical opinion, and routine arrest of doctors is prohibited.
Do I need an expert opinion to file in a consumer commission?
Filing does not strictly require it, but winning almost always does. Commissions give the most weight to opinions from government medical boards or unconnected institutions, covering both the deviation and its causal link to the harm.
How much compensation is awarded for medical negligence in India?
It tracks documented loss: 2026 outcomes ranged from ₹1 lakh for a minor deficiency to ₹2 crore for a wrong-organ surgery, with the Supreme Court's Balram Prasad/Kunal Saha line (₹6 crore plus, 2013) marking the historic high.
Am I entitled to my medical records?
Yes. Hospitals must provide them on request under the professional conduct regulations; a written request with acknowledgment is the correct first step, and refusal itself supports the deficiency case.
Is the hospital liable or only the doctor?
Both can be. Hospitals are vicariously liable for staff and consultants and directly liable for systemic failures such as instrument counts, infection control and absent emergency cover.
Can I complain to the medical council and the consumer commission at the same time?
Yes. The remedies are independent and parallel: licence action in the council, compensation in the commission, and, in gross cases with expert support, criminal prosecution.
This article is for general informational purposes only and does not constitute legal advice. Specific situations need specific counsel.